

ABSTRACT
Results indicated that only a small number of patients were clinically examined before enrolling in and after finishing the treatment, 35%, and 0% respectively. In addition, 15% of patients did not finish their daily PR session (2 to 4.5 hours) in the second step, while 20% of them were not evaluated daily for treatment effectiveness in the fourth step by health workers. Furthermore, 20% of patients did not follow all 6 steps of the Hubbard PR program. Although all CDDs were sufficiently equipped in terms of infrastructure and equipment, the study showed that there remained barriers in implementing the Hubbard PR process, such as the lack of human resources, wasteful usage of equipment, and the lack of technology application for electronic medical records management at the targeted centers. For patients, the difficulties include the lack of awareness and understanding regarding the program, and high temperature during the PR sessions (63%), long PR duration (47%), too many medications and supplements (37%), as well as high cost of treatment (35%). Ensuring adherence and compliance at all steps in the Hubbard PR process can have a positive impact on the health improvement of dioxin patients. To improve the effectiveness and sustainability of this process, we recommended 1) attract and secure high-quality human resources, especially those specialized in physical therapy, 2) develop a plan for effective equipment usage 3) optimize the PR process, 4) apply electronic medical records management to better manage and monitor patients, and 5) improving clinical examination of patients before and after the treatment process at health facilities.
1. INTRODUCTION
According to the latest statistics from UNDP, there are 4.8 million people in Vietnam who were exposed to dioxin [1]. Many studies have shown that dioxin, once pervades the body, can cause complicated damages at multiple sites, leading to several diseases [10, 11]. Current dioxin detoxification methods mainly address symptoms through integrated measures such as improving health with a diet rich in protein, vitamins, stimulating immunity, taking liver supplements to protect liver cells, or taking antioxidants in combination with steaming.
Hubbard purification rundown (PR) is a nonspecialized detoxification method that is being used for the treatment of chronic poisoning and has brought some quite effective results in several countries around the world [2, 14, 15]. This method can expel deeply embedded toxins from tissues, especially adipose tissue, push these into the circulatory system, and dispose of these through the excretory system (mainly through perspiration, urine, feces). Scientific evidence shows that Hubbard PR is capable of reducing the concentration of toxins in the body fat [2, 14, 16]. In Vietnam, the Hubbard PR method was implemented by specialized doctors in the early 2010s. The initial results were highly regarded by those who were exposed to agent orange/dioxin and underwent the treatment [3]. However, there are only individual reports for each patient cohort from the detoxification centers, but no overall researches and assessments of the implementation process, as well as the related advantages and challenges. Therefore, we conducted this study with the purpose to i) Assess the status of Hubbard PR implementation at the detox centers and ii) Analyze the advantages and challenges related to implementation. The results of this research will be the scientific basis for policymakers to provide guidelines for the implementation and expansion of the Hubbard PR method in detoxification centers across the country.
2. RESEARCH SUBJECTS AND METHODS
2.1. Study subject
Subject of quantitative study: Patient management records of those who underwent Hubbard PR, facilities, equipment, and human resources of the process.
Subject of qualitative study: management: board of directors, head doctors at 2 centers for dioxin detoxification (CDDs). Service providers, including doctors and nurses who work directly with victims of agent orange/dioxin. Patients who underwent Hubbard PR at Da Nang and Hanoi’s CDDs
2.2. Study design
This is a cross-sectional descriptive study, combined with qualitative research methods. The qualitative portion was conducted simultaneously with the quantitative portion, to supplement information regarding the advantages and challenges related to the implementation of Hubbard PR at CDDs.
2.3. Sample size
For the quantitative research component, we used the total population sampling method. According to the statistics of the CDDs, a treatment cohort consists of roughly 30 patients, and 1 course of treatment lasts about 21 days. Patients are treated in cohorts and each patient is managed with a medical record from enrollment until the end of the treatment process. Thus, in the first 6 months of 2019, there were about 300 patient records that were inventoried through pre-designed checklists. Among these, one record was deemed ineligible for quantitative analysis. Reports on human resources, facilities, equipment, materials, and documents facilitating the implementation of Hubbard PR at two CDDs of Hanoi and Da Nang were also inventoried through the checklist.
The qualitative research component used purposive sampling to ensure diversity in terms of age, gender, professional qualifications, working positions, number of years of medical work related to non-specialized detoxification sauna. The qualitative sample size includes 14 health workers (HWs) and 30 patients. For the HW group, two CDDs leaders were invited to participate in key informant interviews (KIIs), 12 HW and nurses were invited to participate in two focus group discussions (FGD). Regarding the patient population, 30 were interviewed during KIIs.
2.4. Data collection method
2.4.1. Quantitative data collection
The principal investigator (PI) was the main responsible person for examining medical records and filling out the pre-designed checklists. First, the researcher contacted the leader of the CDDs to obtain approval for data collection and receive data and related reports. After accessing the records, reports, as well as reviewing the facilities and medical equipment, the researcher inventoried books and reports related to patients who underwent Hubbard PR for victims of agent orange/dioxin within the first 6 months of 2019 (from January 2019 to June 2019) and fill in the pre-designed checklist
2.3.2. Qualitative data collection
KII with leaders of CDDS: the principal investigator contacted the leaders of the CDDs to agree on times and locations for KIIs. Each KII lasted 45 to 60 minutes and was recorded after consent was obtained from the subject. Each KII was conducted by the PI and one assistant who was in charge of taking notes and recording. A CDD leader KII guideline was used to guide the interviews.
FGD: the PI contacted the HWs who directly work with the PR treatment at the CDDs to schedule the FGDs. Each FGD lasted about 120 minutes. The PI facilitated the FGDs based on the FGD guideline, with an assistant who took notes and records.
KII with patients: the PI deliberately chose 30 patients who were undergoing Hubbard PR treatment (at the time of the study) from each CDD. Patients who participated in the study were grouped based on their sex and age. After scheduling and agreeing upon a location for the FGDs, the PI recorded the discussions after obtaining their consent and the conduct the interview. Each interview was about 60 minutes long and followed the KII-with-patient guideline.
2.4. Data analysis
The quantitative data were entered using Epidata 3.1 and were analyzed using Stata 14.2. Variables were described through frequency and percentage.
Information from the qualitative portion was transcribed and stored as Word files. The PI read the content of the KIIs and the FGDs to code the information and group them based on themes, using Excel 2016. Several important details of the subject were extracted to demonstrate the results of the study.
3. RESULTS AND DISCUSSION
3.1. Characteristics of subjects
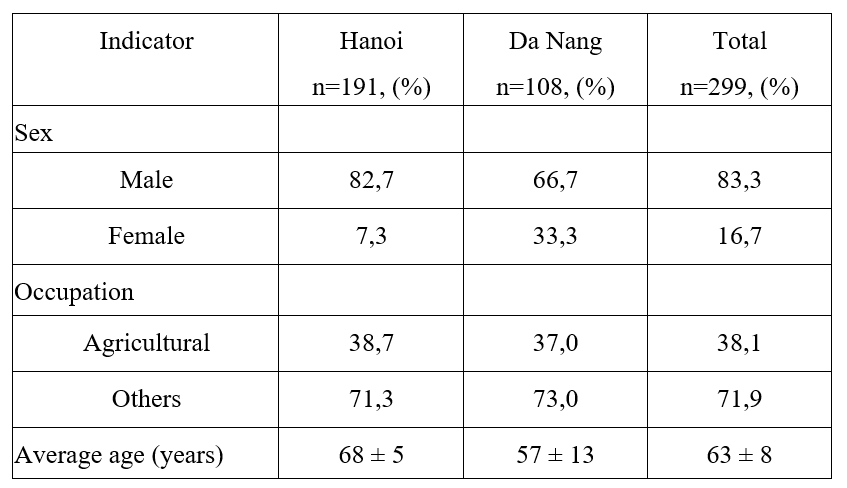
Table 1. General characteristics of patients who underwent Hubbard PR
In
The research was conducted on patients who were exposed to agent orange/dioxin, of old age (63 on average, ranging from 50 to 80 years old). This result is similar to that in studies conducted in Finland, Thai Binh province, or Ha Tinh province [4, 9, 15, 16]. Regarding the sex of patients, 80% of patients who underwent Hubbard PR at 2 CDDs during the first 6 months of 2019 were male. Similar proportions were found in studies conducted by the 103 Military Hospital (70% and 89%) [7]. Regarding patients’ occupation before retirement, about 90% worked non-agricultural jobs (military, governmental, service). A study conducted by Duong Quang Hien has a similar result, with 91% of their patients were military officers and 9% were freelancers [8].
3.2. Current state of Hubbard PR implementation in Hanoi and Da Nang
Figure 1. Proportion of patients examined clinically and sub-clinically before Hubbard PR registration.
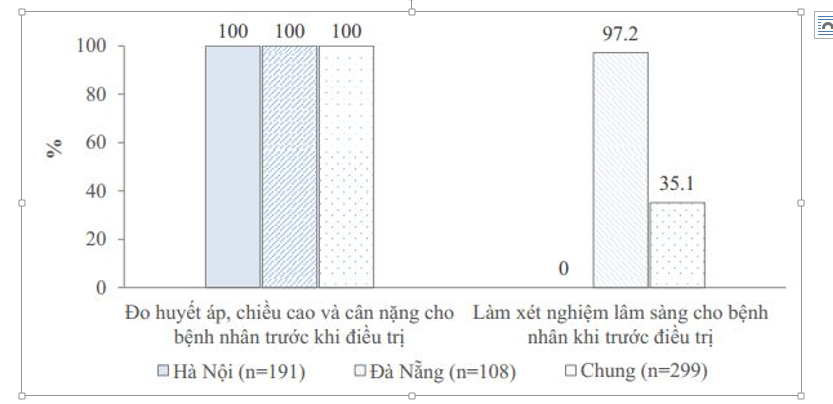 |
The percentage of patients who were not clinically tested at CDDs before registering for Hubbard PR was low, about 35% for both cities, although there was a huge gap between this proportion of Da Nang (97%) and Hanoi (0%). This is because the CDD of Da Nang, while lacks a laboratory department, is located at the city’s center, where patients have access to other medical facilities for testing. In Hanoi, the CDD lacks the personnel for the laboratory department. Thus, there is a need for human resources, along with additional equipment to implement the Hubbard PR process.
However, the pre-treatment assessment of subclinical indicators showed that 100% of patients had their blood pressure, height, and weight measured during the classification step. A similar result is found in the study of Nguyen Hoang Thanh, Duong Quang Hien, Tran Xuan Thu, and Pham Cong Nong [4, 6, 7, 8]. These are the minimum requirement to enrolled in Hubbard PR at our targeted service providers, which are easy to conduct.
Table 2. Patients’ daily exercise, steaming, nutrition supplement, health examination and counseling according to Hubbard PR process.
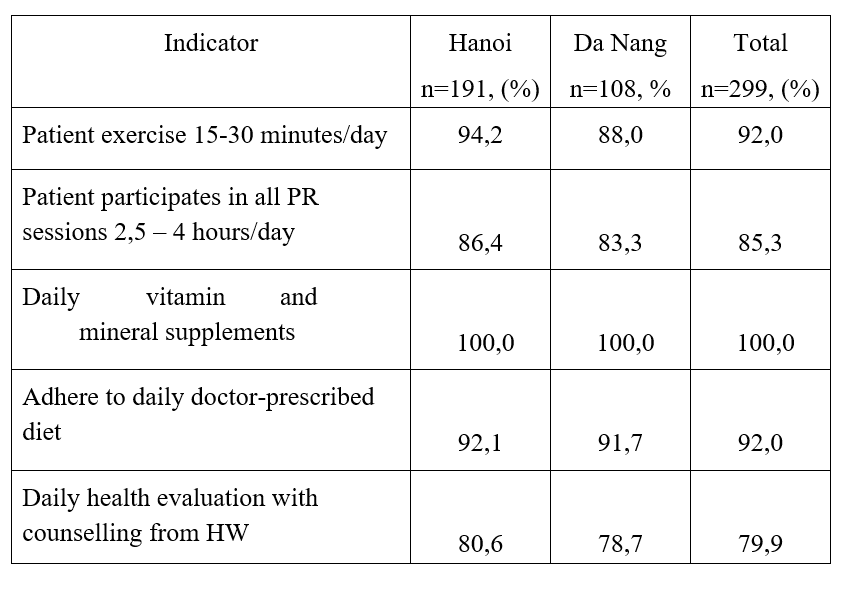
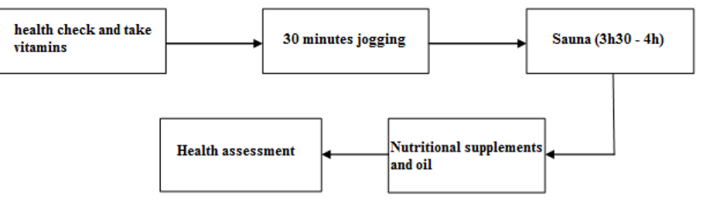
The results of implementing Hubbard PR from steps 2 to 4 showed that the proportion of patients exercised daily for at least 15-30 minutes (step 2); participates in sauna session for 2-4.5 hours (step 3); supplemented vitamins and minerals and complied with prescribed daily diet (step 4) were 92%; 85%; 100% and 92% respectively. This result is similar to a study in Thai Binh but is different compared to the findings from the studies of the Military Medical Academy [4, 7]. Also, patients participating in this study were asked to perform a 4-hour-a-day sauna session, with several cooling baths (every 3 minutes) or rests (5-20 minutes). Meanwhile, patients in the Military Medical Academy’s study only participated in saunas for up to 25 minutes/session with no cooling break in between [7]. A review of different detoxification sauna/steaming methods showed that patients were asked to participate in a sauna with different duration, from 5-30 minutes/session or 30-240 minutes over several times [13]. Another study in the US showed that the duration of the patient's steaming sessions was 14.2 (± 7.5) minutes/session [12]. Therefore, in this study, there were 15% of patients who did not stay in the sauna for the whole duration, which may be due to the temperature of the Hubbard method was higher than that of the traditional method, along with the lack of awareness of patients regarding the treatment requirements and process.
At step 5 in the Hubbard PR process, we found that 80% of the patients were received daily health examinations and counseling throughout the treatment. This result is not found in the study of Nguyen Hoang Thanh and Duong Quang Hien [7, 8]. Although in those studies, HWs did provide counseling and assessment of patients’ condition, this activity was not performed every day. The counseling time was too short to meet patient expectations. This difference is due to each study's purposes. In this study, we are gauging the Hubbard PR compliance. Meanwhile, other studies are interested in the effectiveness of the detoxification steaming method, as shown in the changes of clinical biological indicators.
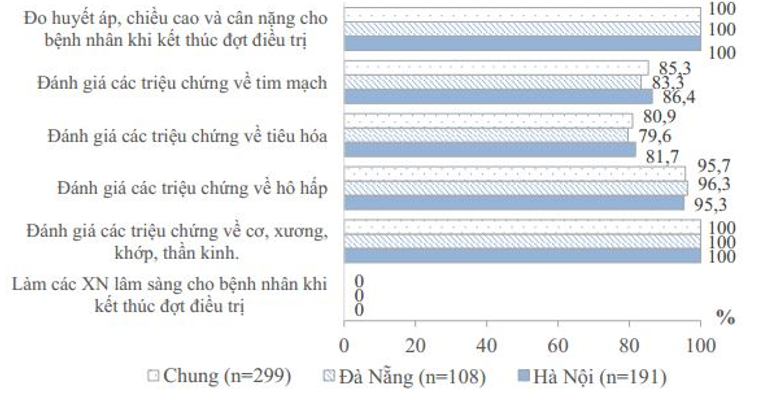 |
| Figure 2. Clinical and sub-clinical evaluation during Hubbard PR of patients and after treatment end |
s
After the treatment, no patient was tested clinically in this study. Meanwhile, this rate in the studies of 103 Military Hospital, Ha Tinh, and Thai Binh CDDs all reached 100% [4, 7, 9]. This difference is because the other studies were designed to evaluate the effectiveness of their intervention, a specialized detoxification sauna method, or to monitor the long-term treatment effectiveness, so the authors focused on assessing the clinical indicators of patients before and after the intervention. Furthermore, the studies of 103 Military Hospital were conducted on small sample sizes (34 and 35 patients) and measured clinical indicators such as ALT enzyme activity, GGT, blood protein concentration [7]. The study in Thai Binh was conducted on 820 patients treated with detoxification sauna in 2 years, each cohort consisted of 28-32 patients [4]. However, this was a well-funded study to evaluate the therapeutic efficacy of the Hubbard PR method before further replication and expansion. Therefore, it is necessary during the classification step is to evaluate the clinical indicators before being enrolled in the treatment. Meanwhile, our study is a cross-sectional study that focused on record management of patients to evaluate the implementation of Hubbard PR. At Hanoi’s CDD, the classification process considered patients’ latest general health examination results as well. Therefore, almost all patients who were enrolled in Hubbard PR treatment during the first 6 months of the year were not clinically tested before enrollment.
| |
| Figure 3. Follow-up on vitamin/mineral supplements and nutritious diet adherence of patients 1 month after the end of treatment |
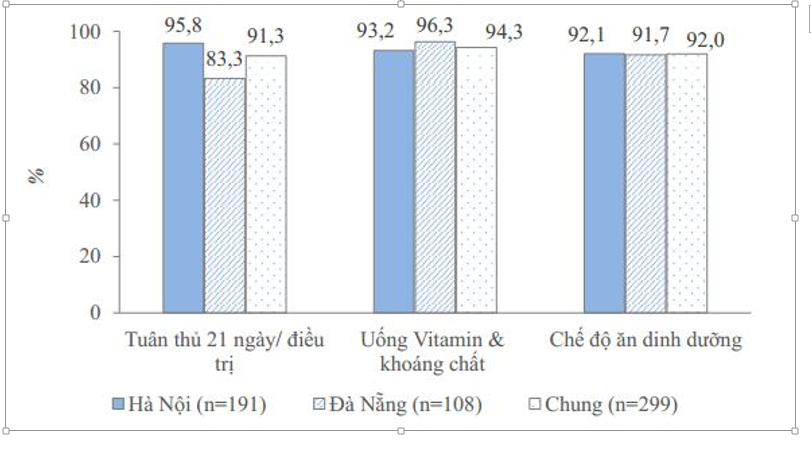
Post-treatment follow-up results showed that the majority (91%) of patients participated in the full 21 days course of Hubbard PR treatment at 2 CDDs. This rate in Hanoi (96%) was higher than that of Da Nang (83%). This may be due to the long duration of the procedure, causing several patients to become ineligible for the treatment. Therefore, it is necessary to optimize the duration of the treatment regimen to encourage patients' full participation, in addition to explaining to the patient about the treatment process. The percentage of patients who complied with the vitamin/mineral and diet recommendation after treatment was similar between Hanoi and Da Nang: 93% with 96% and 92% with 92%. Adherence to nutrition regimens and gradual reduction of medication after treatment helps to enhance and maintain patients’ health condition after treatment.
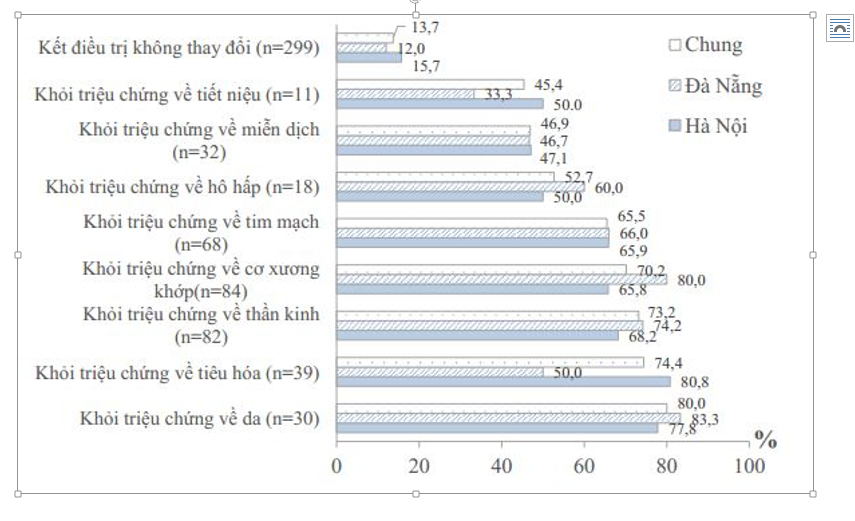 |
| Figure 4. The effectiveness of Hubbard PR treatment with patients |
On the effectiveness of Hubbard PR treatment, the results showed that for patient’s with skin diseases, neurological disease, musculoskeletal disease, digestive diseases, cardiovascular disease, the proportion of patients whose symptoms were improved were 80%, 73.2%, 70.2%, 74.4%, and 65.5% respectively. Patients with the renal and urinary disease had the lowest proportion of improvement (45.9%). This result is similar to the results of Nguyen Xuan He: 92% of patients with cardiovascular diseases, 76% of patients with mental diseases/disorders saw improvement [9]. According to the VAVA report in the Thai Binh province, symptoms that improved the most were: limb numbness, osteoarthritis pain, insomnia headache, hypertension [4].
The proportion of patients who did not see any changes or felt more tired after treatment was 13.7% (15.7% in Hanoi and 12% in Da Nang). This may be because the
patient did not adhere to the nutrition and medication regimen, thus feeling tired while participating in the sauna. Therefore, it is necessary to strictly monitor and control the vitamins and minerals supplements and diet of patients, while developing a specific exercise regimen and diet suitable for each patient.
3.3. Challenges in implementation of Hubbard PR
3.3.1. Human resources
KII with CDDs’ leaders and FGDs with HWs showed that the current human resources for Hubbard PR operation remained scarce. The total number of HWs at both CDDs was 16, which was not sufficient. Therefore, one person had to be responsible for multiple positions during the treatment process. This could be explained by the current benefits and salary, which were not appropriate for attracting high-quality personnel. Meanwhile, at private practices and service providers, the benefits and salary were more well-received compared to that of the CDDs. Therefore, to ensure the appropriate human resources for the process, the CDDs need to have plans for additional hiring and improving the current benefits and salary for employees.
Regarding the quality of the human resources, the current state at the CDDs was not sufficient, as the CDDs had become operational for only a short amount of time, as well as some HWs lacks work experience or the lack of good benefits and salary package to attract high-quality professionals. All of these contributed to a lack of high- quality professionals. Despite the lack of facilities, equipment, and human resources, the HWs were enthusiastic, passionate, and creative in their jobs. To better the human resource’ quality, the CDDs should organize panel discussions on medical specializations between HWs from the CDDs and other facilities, inviting experts to work as consultants at the CDDs, improve the benefits/salary to attract high-quality professionals, and organize capacity building sessions for HW while encouraging HWs to self-learn and self-development their technical capacities.
3.3.2. Facilities, equipment, and medical material
The initial facilities and equipment were sponsored by various funds to ensure the initial basic operation of the CDDs. However, each CDD needs to have their plan for maintenance that is suitable for the current situation, while developing a strategy for expansion in order to meet the increasing demand.
3.3.3. Financial factor
All CDDs depend on 2 main sources of funding, one from the Social Protection Centers of the Department of Labor, Invalids and Social of provinces/cities, and the other source from socialization, funded by businesses, organizations, and individuals’ donations. However, this source of funding is often used for travel and allowance expense of treatment participants. With such limited fundings, it is difficult to repair, maintain, and purchase new equipment, as well as attracting and fostering high-quality human resources. Therefore, the leaders of the CDDs have proposed to develop a plan to establish a branch for general population service, those who are not agent orange/dioxin victims (chemical poisoning, occupational hazards, heavy metal poisoning, heroin addiction...) to increase funding for each center
3.3.4. Technology application
The CDDs were not equipped with electronic medical records management software, so there were still many difficulties in managing and monitoring patients. Besides, there were not enough human resources to operate the system. Therefore, in the future, it is necessary to sufficiently secure human resources and electronic equipment.
3.3.5. Management and related documents
The CDDs are under the provincial Association of Agent Orange Victims and operate based on the counseling of the Department of Health, following the guidelines of the City People's Committee. The CDD is responsible for performing steaming, detoxification, rehabilitation, and health improvement for victims of agent orange/dioxin and other poisoned patients. With such a structure, the CDD can easily update on the policies, guidelines, and operating policies of the association as well as obtain the necessary information of the subjects involved in the detoxification. Strict organizational structure, units operating in one process under the direction of the Board of Directors leads to high professionalism and ease in implementing the PR process.
Management efficiency was not optimal, due to the lack of human resources. The solution to overcome this is to develop recruitment plans and attract high-quality human resources.
Although the CDDs have Hubbard PR implementation guidelines, the documents were not localized to be suitable with the current conditions of the CDDs. Therefore, the CDDs need to develop a set of instructions to suit the local conditions.
3.3.6. Patient-related factors
The results of patient KIIs showed that patients were mainly introduced by health workers at the CDDs, and the level of knowledge about Hubbard PR was limited, which may be due to the lack of promotion and publicity. In this regard, the CDDs should cooperate with the Central Association of Agent Orange/Dioxin Victims to introduce, advertise Hubbard PR using media (newspaper, radio, internet…), organize seminars and conferences for victims of agent orange/dioxin, and the community.
Most of the patients interviewed considered the Hubbard PR method as effective and suitable for agent orange/dioxin victims. The Hubbard PR method was developed based on the principle of detoxification through sweat, digestion, and urology while combining additional vitamins and minerals to improve health. Meanwhile, victims of dioxin often suffer from chronic diseases that affect their health, so this method is very suitable for the subjects.
During the implementation of Hubbard PR, some advantages were the enthusiastic, thoughtful and creative attitude of HWs. In addition, Hubbard PR was also trusted by the patient's family members. This is one of the advantages that helped patients and health workers share difficulties in the treatment process. In addition, a number of patients thought that Hubbard PR was quite simple and easy to implement.
However, there were still some difficulties in the process of Hubbard PR, such as excessive temperature, dose of drugs, and exercise. This may be due to the fact that patients were mostly elders and were suffering from many associated chronic diseases. Therefore, the initial classification of health and development of the Hubbard PR for each subject is very important. In addition, some patients felt that the duration (21 days) was relatively long for them because, in addition to steaming, patients were also periodically examined for other chronic diseases (hypertension, diabetes mellitus, COPD...); and, patients found themselves feeling relatively well after about 10-14 days. Therefore, many patients suggested shortening the treatment time, to ensure continuous treatment.
4. CONCLUSION
Regarding the implementation of Hubbard PR, although the CDDs and the majority of patients have followed the instructions, the proportion of patients receiving clinical tests before and after treatment was quite low, respectively 35% and 0%. The proportion of patients who did not participate in all PR sessions with a duration of 2-4.5 hours/day was 15%, nearly 20% of them were not evaluated by doctors using questionnaires after each day of treatment. In addition, nearly 20% of patients did not adhere to 6 steps of the process. Regarding adherence to diet and vitamin intake after the end of treatment 1 month, the percentage of patients who complied with taking vitamin and mineral supplements was 94%. Lastly, 92% of them complied with the daily diet of vegetables, fruits, and protein.
For CDDS, the barriers in the implementation of Hubbard PR include inappropriate human resources, unattractive benefits, and salary, inappropriately designed and deteriorating saunas, inefficient use of equipment, or the lack of equipment for indoor exercise, or long time for drugs transfer from the central to local branches. In addition, there was a lack of applying of technology and electronic medical records management at the CDDs, which brought many shortcomings due to the lack of manpower to operate and manage the system. Currently, there is no specific guideline issued by the MOH or the Provincial Department of Health to guide CDDs on how to implement Hubbard PR.
For patients, there were also challenges, such as the lack of understanding of the treatment or patients not adhering to the treatment regimen. In addition, some other complaints were: PR temperature too hot (63%), long PR session duration (47%), too many medications taken during treatment (37%), and the cost of treatment is too expensive (35%).
5. RECOMMENDATION
The benefits of the Hubbard PR approach in improving subclinical symptoms of agent orange/dioxin patients have been found in studies around the world and in Vietnam. To further improve the effectiveness of the treatment, the compliance of health workers and patients in CDDs with the implementation of Hubbard PR plays a very important role. Therefore, for CDDs, they need to i) strengthen and reallocate human resources with expertise in physiotherapy, ii) plan for effective use of equipment as well as additional indoor exercise equipment for the treatment regimen, iii) optimize the detox PR process, shortening the session duration, increase break duration with written instruction from MOH and Provincial Dept. of Health, iv) develop electronic medical record management software for east of management and monitoring of patients’ health, and v) perform clinical assessments of patients before and after treatment at the CDDs. For patients, it is necessary to communicate with them about the treatment and its benefits, adherence requirements of Hubbard PR before enrolling in treatment.
REFERENCES
Ministry of Natural Resources and- UNDP (2015), 50 questions and answers about Agent Orange/dioxin.
Mai Nam, Vo Dinh Khuynh (2014), Results of the implementation of the National Criteria for Commune Health in 2013 (period 2011 - 2020).
Nguyen Van Tuong (2010), Evaluation of changes in some hematological and biochemical parameters in exercise subjects according to the improved Hubbard procedure, Hanoi Medical University.
Vo Ha (2008), Non-drug treatment, Oriental Publishing House.
The Scientific Committee of the Central Association and the Association of Victims of Agent Orange - Dioxin in Thai Binh Province (2016), Survey, evaluate the effectiveness and cost of treatment to improve the health of people infected with Agent Orange by the Hubbard detox sauna, Ha Noi
Nguyen Hoang Thanh et al. (2015), Evaluation of non-specific detoxification effectiveness in people exposed to Agent Orange/dioxin at 103 Military Hospital, Journal of Military Medicine and Pharmacy, 1, 98-103.
Duong Quang Hien (2017), Study on the safety and effectiveness of detoxification of the method “GD-103” on people exposed to Agent Orange/dioxin.
Nguyen Xuan He (2015), Detoxification according to the Lerol Huberd method, Ha Tinh.
Institute of Medicine (2014), "Veterans and Agent Orange: Update 2012", 2014: Washington DC.
Andrey A Panteleyev David R Bickers (2006), "Dioxin‐induced chloracne– reconstructing the cellular and molecular mechanisms of a classic environmental disease", Experimental dermatology. 15(9), 705-730.
CG Maulfair (2005), Sauna detoxifi cation of metals, pesticides and chemicals: Addressing the background exposures and increasing health problems of an industrial society, New York,
Cochrane Systematic Review (2005), "Inpatient versus other settings for detoxification for opioid dependence".
Joy Hussain and et al (2018), "Clinical Effects of Regular Dry Sauna Bathing: A Systematic Review", PubMed access
Kunutsor SK. (2018), Sauna bathing reduces the risk of stroke in Finnish men and women: A prospective cohort study.
T. Laukkanen (2018), "Sauna bathing is associated with reduced cardiovascular mortality and improves risk prediction in men and women: a prospective cohort study", BMC Med. 16(1), 219.
1) Center for high-tech research and treatment, Tropical Medicine Academy, Center of Vietnam Russia Tropical Medicine
2) Vietnam Association for Victims of Agent Orange
%20nh%E1%BA%ADn%20c%E1%BB%9D%20thi%20%C4%91ua%20xu%E1%BA%A5t%20s%E1%BA%AFc%20n%C4%83m%202025_thumb_720.jpg)



_thumb_720.jpg)


_thumb_720.jpg)










.jpg)









Comment